99% Translated
0% Upvoted
1 Translations, 0 Upvotes, Last Activity 2 months ago
1 Translations, 0 Upvotes, Last Activity 2 months ago
1 Translations, 0 Upvotes, Last Activity 2 months ago
1 Translations, 0 Upvotes, Last Activity 2 months ago
1 Translations, 0 Upvotes, Last Activity 2 months ago
1 Translations, 0 Upvotes, Last Activity 2 months ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 2 weeks ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month, 1 week ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
0 Translations, 0 Upvotes, Last Activity None
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
1 Translations, 0 Upvotes, Last Activity 1 month ago
Essential Tremor and Modern Treatment Options: From Medication to MR-Guided Focused Ultrasound.
For many people, the first signs of tremor appear gradually and almost innocently. A hand shakes slightly while holding a cup of coffee. Handwriting becomes less steady. Soup spills from a spoon. Friends or family members begin noticing a subtle quiver in the voice or a shaking hand during conversation. At first, these symptoms may seem like ordinary aging, nervousness, fatigue, or stress. Over time, however, the tremor may slowly worsen until routine daily activities become frustrating, embarrassing, or even impossible.
The most common serious tremor disorder is Essential Tremor (ET), a neurological condition affecting millions of people worldwide. Although long considered a relatively benign disorder, physicians now recognize that severe essential tremor can profoundly affect quality of life, emotional well-being, and personal independence. In recent years, major advances in treatment — particularly magnetic resonance-guided focused ultrasound (MRgFUS) — have transformed the outlook for many patients whose symptoms no longer respond adequately to medication.
Essential tremor most commonly affects the hands and arms, although the head, voice, jaw, and legs may also be involved. Unlike Parkinson’s disease, where tremor is often most noticeable while the body is at rest, essential tremor usually appears during activity. The tremor becomes more evident while writing, eating, drinking, shaving, sewing, typing, or holding objects. Patients often notice that stress, anxiety, fatigue, or caffeine make the shaking worse. Many also observe that small amounts of alcohol temporarily reduce the tremor, a feature that can help distinguish essential tremor from other movement disorders.
The severity of the condition varies enormously. Some individuals experience only mild inconvenience throughout life. Others gradually become unable to sign their names legibly, carry a plate across a room, or drink from a glass without spilling. Patients frequently describe the social consequences as almost worse than the physical disability itself. Tremor may draw unwanted attention in restaurants, meetings, or social gatherings. Many patients begin avoiding public meals, social functions, or hobbies they once enjoyed. The emotional burden can include embarrassment, frustration, anxiety, and increasing social withdrawal.
Doctors still do not fully understand the exact cause of essential tremor. Research suggests that abnormal signaling develops within brain circuits involving the cerebellum, thalamus, and motor pathways that coordinate movement. There is also a strong hereditary component in many families, and roughly half of patients report relatives with similar tremor symptoms. Essential tremor is therefore increasingly understood as a genuine neurological disease rather than merely a nuisance associated with aging or nervousness.
Diagnosis is usually made clinically by a neurologist. There is no single blood test or brain scan that definitively confirms essential tremor. Instead, doctors rely on the pattern of symptoms, neurological examination, and exclusion of other causes. Essential tremor typically presents as a bilateral action tremor affecting both hands over a period of years. Patients generally do not display the marked slowness, rigidity, or shuffling gait characteristic of Parkinson’s disease.
Parkinson's Disease, although also associated with tremor, represents a very different neurological condition. Parkinsonian tremor is classically strongest at rest and is accompanied by other symptoms including muscular rigidity, slowed movement, stooped posture, reduced facial expression, and gait disturbance. Nevertheless, some patients with Parkinson’s disease suffer from severe tremor that remains disabling despite otherwise adequate medication control. For these patients, modern tremor procedures may also play an important therapeutic role.
Treatment for essential tremor usually begins conservatively with medication. The two principal first-line drugs are Propranolol and Primidone. Propranolol, a beta-blocker originally developed for cardiovascular disease, often reduces tremor amplitude by roughly 40–50%. Many patients experience worthwhile improvement, particularly early in the disease. However, side effects such as fatigue, dizziness, low blood pressure, depression, or exercise intolerance may limit its usefulness, especially in older adults or patients with asthma or cardiac disease.
Primidone, originally an anti-seizure medication, can be similarly effective and occasionally even more beneficial than propranolol. Yet it too carries limitations. Patients commonly report drowsiness, dizziness, imbalance, nausea, or mental fogginess, particularly during dose escalation. Some older patients find the medication difficult to tolerate at fully therapeutic doses. Additional drugs such as topiramate, gabapentin, benzodiazepines, or botulinum toxin injections may provide benefit in selected cases, but medication therapy remains imperfect overall. Many patients eventually reach a point where either tremor control becomes inadequate or medication side effects become unacceptable.
For patients with severe medically refractory tremor, surgical therapies may then be considered. For several decades, the dominant advanced treatment has been Deep Brain Stimulation (DBS). In DBS surgery, electrodes are implanted into specific regions deep within the brain, most commonly the ventral intermediate nucleus (VIM) of the thalamus. The electrodes are connected to a pulse generator implanted beneath the skin of the chest, somewhat analogous to a cardiac pacemaker. Electrical stimulation modulates abnormal tremor circuits and can dramatically reduce tremor severity.
DBS is highly effective. In many patients, tremor reduction ranges from 60–90%, often restoring substantial functional independence. Unlike older lesioning procedures, DBS is adjustable and reversible in its stimulation effects. Physicians can fine-tune stimulation parameters over time as symptoms evolve. Bilateral treatment is also feasible. However, DBS still requires invasive neurosurgery, implanted hardware, periodic battery replacement, and long-term device programming. Risks include infection, bleeding, hardware malfunction, and the burdens associated with chronic implanted systems.
The emergence of Magnetic Resonance-guided Focused Ultrasound Thalamotomy has therefore attracted enormous interest. MR-guided focused ultrasound represents one of the most important recent advances in functional neurosurgery because it offers a way to create a therapeutic brain lesion without opening the skull or implanting hardware.
The technology combines several innovations simultaneously. Hundreds of ultrasound beams are directed through the intact skull and focused precisely on a tiny target within the thalamus. Individually, the ultrasound beams pass harmlessly through tissue. At the focal point, however, the combined energy generates enough heat to create a highly localized thermal lesion that interrupts abnormal tremor circuitry. The patient lies within an MRI scanner during the procedure, allowing physicians to visualize the brain in real time and monitor tissue temperature continuously using MRI thermometry.
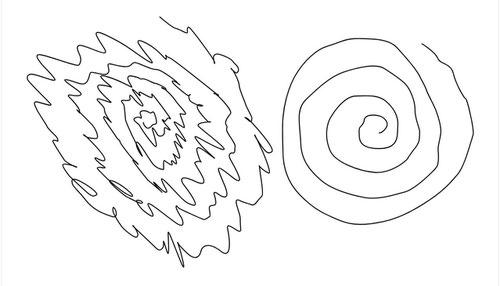
One remarkable aspect of MRgFUS is that patients remain awake during treatment. After low-energy test sonications confirm targeting accuracy, progressively stronger treatments are delivered while doctors repeatedly assess tremor improvement and monitor for side effects. In many cases, patients observe immediate improvement during the procedure itself. Some are able to draw smooth spirals or hold a cup steadily for the first time in years while still inside the MRI scanner.
In 2016, the U.S. Food and Drug Administration approved unilateral MRgFUS thalamotomy for medication-refractory essential tremor. Subsequent studies demonstrated substantial tremor reduction, commonly in the range of 50–75%, along with major improvements in quality of life and daily functioning. The procedure is entirely incisionless, generally performed in a single day, and avoids implanted hardware altogether. For many patients — particularly older individuals who prefer to avoid open surgery — this represents an extremely attractive option.
No procedure, however, is entirely free of risk. Temporary side effects after MRgFUS may include numbness, tingling, imbalance, unsteady gait, or mild speech difficulty. Most improve over time, but some symptoms may persist. The greatest concern historically has involved bilateral treatment. Earlier generations of bilateral thalamotomy performed with radiofrequency lesioning sometimes produced serious speech and balance complications. As a result, modern MRgFUS bilateral treatment is approached cautiously using a staged strategy.
Essential tremor commonly affects both hands, and many patients remain significantly disabled after only one side is treated. Modern staged bilateral MRgFUS addresses this problem by treating one side first, then waiting several months before considering treatment of the opposite side. This delay allows physicians to assess recovery, gait stability, speech, swallowing, cognition, and overall benefit before proceeding further. Current practice generally requires an interval of at least nine months between procedures.
Recent studies of staged bilateral MRgFUS have shown highly encouraging results. Many patients experience major additional functional improvement after second-side treatment, particularly in eating, dressing, writing, and personal care activities. Overall tremor reduction commonly reaches 60–80% with substantial gains in quality of life. Most side effects remain mild and manageable, although gait imbalance and speech difficulties continue to require careful monitoring. Patients who develop significant residual imbalance or dysarthria after the first procedure are generally not considered ideal candidates for second-side treatment.
An important practical question for many patients concerns medication use after treatment. Following successful MRgFUS, some patients reduce or discontinue tremor medications entirely, especially after bilateral treatment. Others continue lower doses because residual tremor persists or because medications still provide additional benefit. Patients with Parkinson’s disease usually continue broader Parkinsonian medications even if tremor improves substantially, since focused ultrasound primarily addresses tremor rather than the entire disease process.
As of 2026, MR-guided focused ultrasound has established itself as a major therapeutic advance for severe tremor disorders. It does not cure essential tremor or Parkinson’s disease, nor does it eliminate all risk. Nevertheless, for carefully selected patients whose lives have become dominated by disabling tremor, MRgFUS offers something that until recently seemed almost impossible: meaningful tremor reduction through a precise, incisionless outpatient procedure guided in real time by modern imaging technology. For many patients, the result is not merely less shaking, but a restoration of confidence, independence, and participation in everyday life.
Image - Archimedean spirals drawn by a 22-year-old male suffering with unilateral essential tremor. The spiral on the left was drawn by the subject using his left hand, and the one on the right with his right hand.
Source: https://upload.wikimedia.org/wikipedia/commons/d/d1/Spiral_drawing_of_Essential_Tremor_patient.svg .
https://creativecommons.org/licenses/by-sa/4.0/
MvR, May 25, 2026 – With assistance of ChatGPT. ✍️